Key takeaways:
~ The gut mucosal barrier is a vital and underappreciated part of our overall health and wellness.
~ The mucus layer protects us from bacteria, viruses, toxins, and our own digestive enzymes.
~ Genetic variants in the mucus production genes can impact the risk of certain diseases.
~ Our modern diet is full of emulsifiers that thin out our gut mucosal barrier, leading to increased inflammatory response in the gut.
Digestion and Protection: Gut Barrier
From the mouth through the end of the digestive tract, you have a surface area of about 32 m2 of epithelial cells covered by a mucosal barrier. The epithelial cells make up a skin-like barrier, with cells tightly joined together. But the cool part that keeps all of this working – and all of us alive – is a layer of mucus covering and protecting us.[ref]
The gut mucosal layer is a barrier of mucus that prevents digestive enzymes, bacteria, acid, and other things in the intestines from coming into contact with the epithelial cells lining your intestinal tract.
Small molecules, like amino acids, sugar, minerals, and vitamins, can pass through the mucosal barrier and then are absorbed into the body. So the foods you eat get broken down by powerful digestive enzymes into small components (amino acids, sugars, fatty acids) that can pass through the mucosal barrier and be absorbed into the body. But the powerful digestive enzymes, gut bacteria, and toxins are kept out of the body.
Why is this important for overall health?
Degradation or thinning of the mucosal barrier is linked to:[ref][ref][ref][ref][ref][ref]
- autoimmune disease
- inflammatory bowel disease (IBD)
- obesity
- metabolic disorders
- heart failure
- organ failure and death
Let’s dive into the details of this unsung (and slimy) hero… and then go into how and why our modern diet is washing away the mucosal barrier.
Mucosal layer:
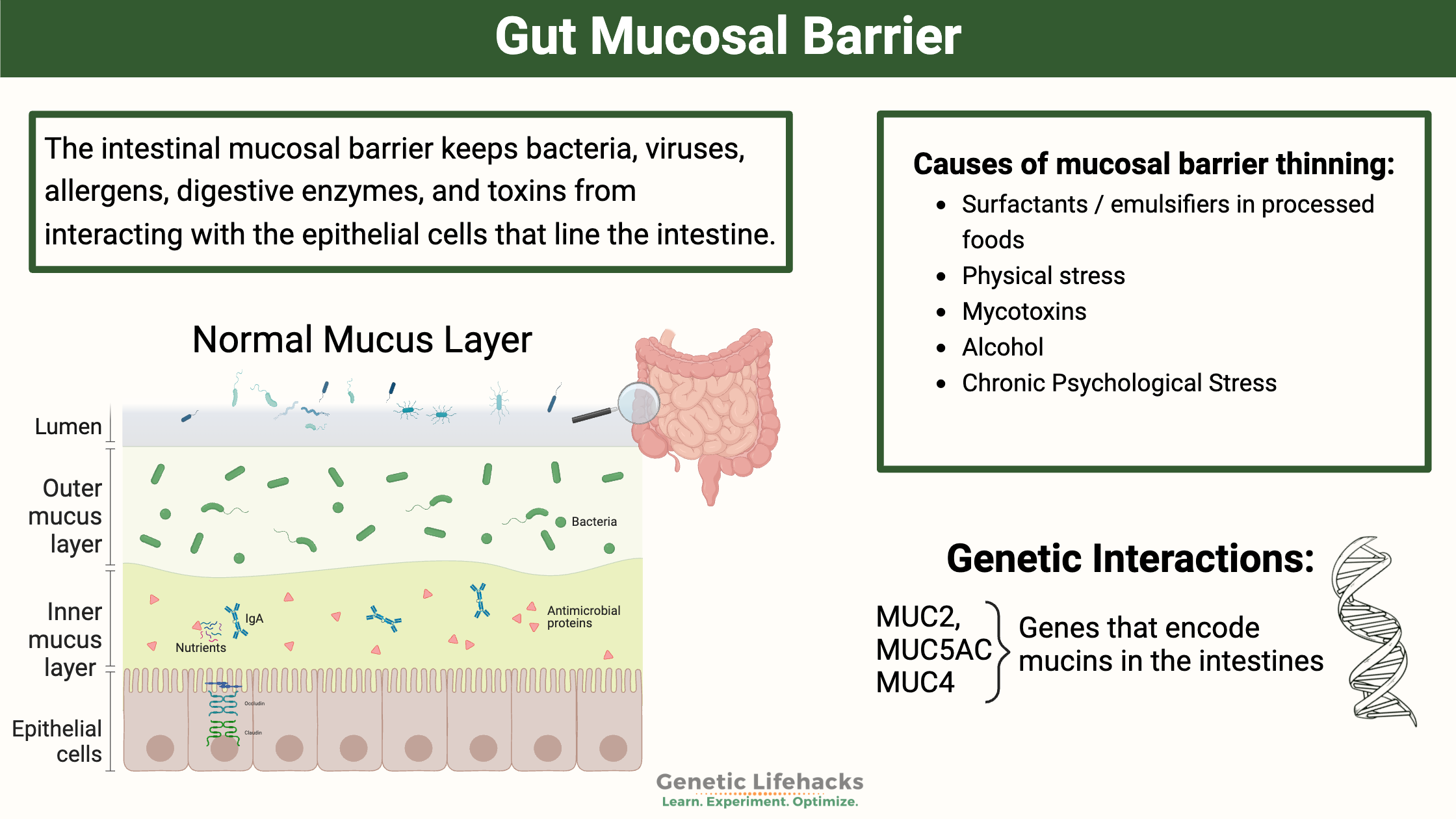
The intestinal mucosal barrier keeps bacteria, viruses, allergens, and toxins from interacting with the epithelial cells that line the intestine. It separates your body from “the outside” – food, microbes, bad stuff. The lining is constantly being built and shed. This constant flux means that any microbes or parasites trapped in it can be moved out of the body.[ref]
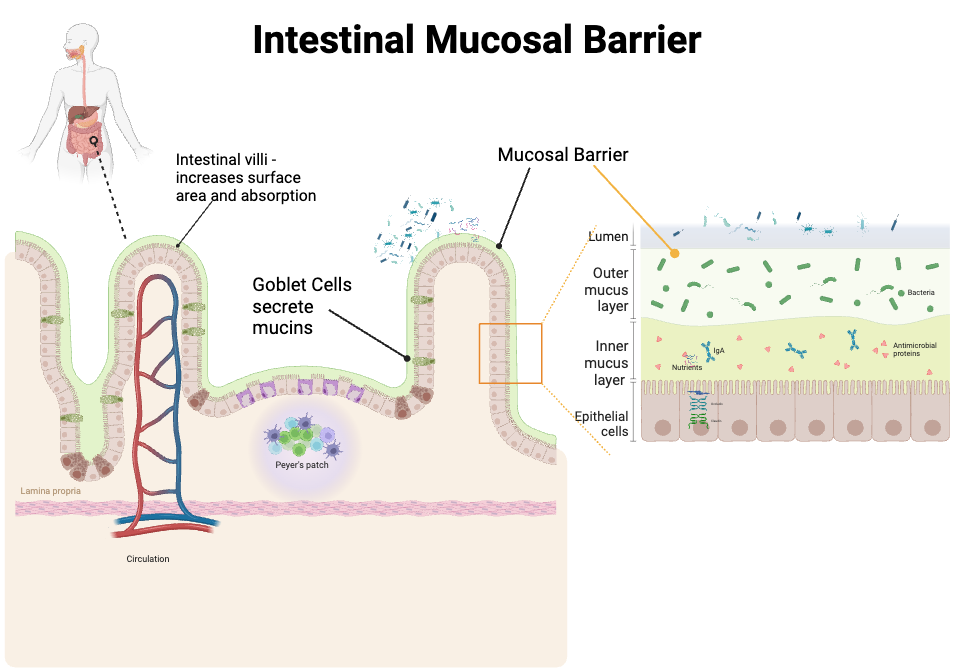
This mucus layer is made up of large, glycosylated proteins called mucins that form a thick, slimy protective layer. Mucins are secreted by specialized intestinal cells called goblet cells. The mucins interact with water to form a gel layer along the entire length of the digestive tract.[[ref] Within this mucosal barrier, about 95% is water, and the rest is made up of the gel-forming mucins as well as cellular debris from your intestinal cells as they shed (your intestines are constantly forming new cells, turning over every few days).[ref]
Different mucins are found to predominate in different mucosal barriers, such as in the nose, lungs, and stomach. In the intestines, MUC2 and MUC5A2 are the primary mucins.[ref] Other mucins, such as MUC4, can act to anchor the mucin to the epithelial cells in the colon.[ref]
The mucosal barrier is a bit different in the small intestines compared to the colon. In the colon, there is a thicker mucosal layer that is anchored to the epithelium along with a relatively looser outer layer of mucus. This is due to a higher microbial burden in the colon which therefore requires a thicker barrier along with the looser layer that is constantly being shed.[ref]
Here’s a diagram to explain further what the mucosal layer looks like:
Let’s take a look at some of the specific genes that encode the mucins in the intestines.
MUC2 (Mucin 2) gene:
As I mentioned earlier, the MUC2 gene encodes one of the primary mucins that make up the intestinal mucosal barrier.[ref] (It’s also found as a component of other mucosal areas in the body as well, such as in the endometrium.)
MUC2 is constantly being secreted by goblet cells in the intestine, and some of it remains anchored to the intestinal mucosa.[ref]
MUC2 and other mucins are upregulated to increase mucin production in response to inflammation and also in a daily rhythm in response to bile acid secretion for digestion, which also breaks down mucins. This is a natural system that is constantly being balanced – production increases when the barrier is threatened or compromised.[ref]
In animal studies, reduced MUC2 gene expression causes less MUC2 production. This results in inflammation in the gut due to gut bacteria being in closer contact with the epithelial cells lining the gut.[ref]
MUC5AC (Mucin 5AC):
The other main component of intestinal mucus is MUC5AC. In IBD, MUC5AC is increased in response to active inflammation. It is thought that this is a tissue-protective response since the same type of increased production happens in helminth infections.
Animal studies show that a deficiency of MUC5AC can increase the risk of IBD and the intestinal inflammation seen in IBD.[ref]
The mucosal barrier protects us from digesting ourselves:
There is a new study (Oct. 2024) that proposes a theory of why we have inflammation, dysregulation of cell function, and a general breakdown of tissue when we get old. In a nutshell, the researchers show (in animals) that digestive enzymes are escaping the intestines and wreaking havoc in the body by damaging tissues in aging due to a thin mucosal barrier. The study showed that the mucosal barrier thins in aging, which allows higher amounts of strong, protein-degrading digestive enzymes to come into contact with the intestinal epithelial cells. These digestive enzymes then can damage the intestinal cells and make it through to circulate in the body. The study showed that the digestive enzymes then accumulate in the organs and cause cell damage. [ref – open access, worth reading]
The study built upon older studies that showed that multiple organ failure from shock is actually caused by the pancreatic digestive enzymes entering the circulation and causing enough organ damage to cause death.
Thus, your gut mucosal barrier literally keeps you alive!
The mucosal layer interact with the microbiome:
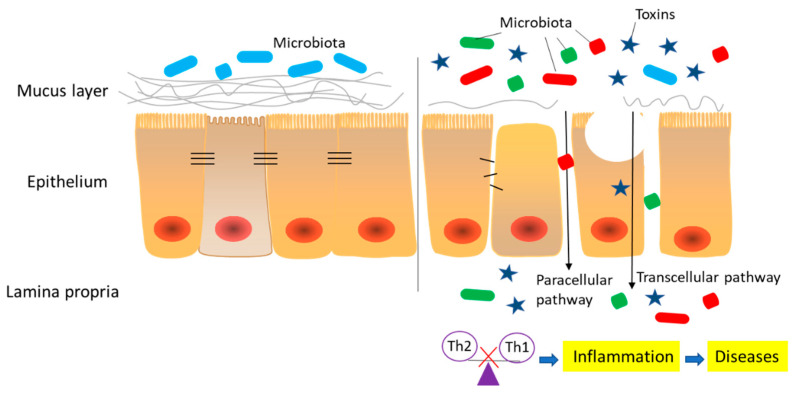
The mucosal layer provides a physical barrier to prevent gut microbes from coming into contact with the epithelial cells. Bacteria can be trapped in the mucosa, sloughed out, and excreted in feces.
Mucins contain glycoproteins which can be used by some bacteria as food. Yes, bacteria are currently munching on your intestinal mucosal layer. This is normal, when in balance.
However, the overgrowth of certain gut bacteria can degrade the mucosal barrier. For example, certain strains of E. coli have been shown specifically to degrade the MUC2 mucin barrier. Akermensia muciniphilia is another mucin-degrading bacteria, and higher levels of certain A. muciniphila species are linked to inflammatory bowel diseases. One theory is that IBD is due, at least in part, to decreased mucosal barrier and increased intestinal inflammation due to the translocation of bacteria close to the epithelial cells.[ref][ref]
Studies show that when dietary fiber is low, the microbes that normally survive on dietary fiber may switch to consuming the glycoproteins in the mucosal barrier.[ref] The microbiome is a balancing act of having the right microbes, the right amount of fiber, and a healthy mucosal barrier.
Causes of mucosal barrier thinning:
The mucosal layer is constantly being generated by goblet cells in the intestines. This is a dynamic, changing landscape that is affected by food, the gut microbiome, inflammation or damage in the intestines, and overall health.
Let’s take a look at how the foods we eat and the toxins that we are exposed to can damage the mucosa.
Surfactants and emulsifiers in processed foods:
Emulsifiers and surfactants are ubiquitous in processed foods. You may be wondering why surfactants – which most people associate with laundry detergent or dishwashing soap – are in foods. Surfactants and emulsifiers make the texture of low-fat dairy products (or non-dairy substitutes) creamy, improve the shelf stability of baked goods, and keep pickles crunchy.
The addition of surfactants started back in the 1930s with mono- and diglycerides being used to formulate margarine. Then in the 1960s, a new bread processing technique was developed for commercial bread production that included surfactants to interact with wheat and oils in the production of a shelf-stable product. Non-ionic surfactants are used as emulsifiers, dough stabilizers, and aerating agents. These same surfactants are also used in pharmaceuticals to increase absorption by breaking down the intestinal barrier.[ref]
Surfactants work by interacting with nonpolar interfaces and lowering the water-repellent activity of the surface. Some surfactants break the bonds within the mucus gel, and some can interact with the phospholipid bilayer on cells.[ref] Think about the way that dish detergent breaks up oil or how certain surfactant cleaners are great at cleaning up slimy, sticky stuff.
A 2018 study found that two emulsifiers, carboxymethylcellulose and polysorbate 80 (Tween 80), cause alterations to the thickness and amount of mucous in the intestinal barrier. The emulsifiers also changed the structural properties of the mucus.[ref] Many other studies back up these findings as well as showing that a few other emulsifiers also alter the mucosal barrier. For example, β-lactoglobulin (β-lac) which is derived from whey protein also changes the permeability of the mucosa.[ref]
Taking this one step further, polysorbate 80 as a dietary emulsifier has been shown to decrease the expression of MUC2. It also increases the intestinal absorption of phthalates from microplastics.[ref][ref]
Research also shows that emulsifiers, specifically polysorbate 80, cause impaired glycemic tolerance, increased gall bladder size, and reduced intestinal mucosa thickness. The reduced mucosal thickness causes intestinal bacteria to be closer to the epithelial cells and increases inflammation.[ref]
Related article: Leaky Gut, Emulsifiers, and Inflammation
Mycotoxins: Toxins from mold directly damage the mucosal barrier
Mycotoxins are the toxic metabolites produced by mold and are often a problem in contaminated food. Research shows that mycotoxins in food can thin the mucosal barrier and disrupt the gut by causing inflammation.
We get mycotoxins from different food sources such as peanuts, which are often contaminated with aflatoxin, grain products that have been improperly stored, and even some coffees. Essentially anything that is grown in a region prone to mold can end up contaminated with mycotoxins, including the grain fed to cows who can then pass the mycotoxins through their milk. Don’t get me wrong – not all food is contaminated with mycotoxins, but for some foods, like peanuts, it can be a real problem.
Related article: Mycotoxins, mold, and your genes
When it comes to the mucosal barrier and the epithelium in the intestines, mycotoxins have been shown in hundreds of studies to cause damage. With the epithelial barrier, mycotoxins cause a loosening of tight junctions and an increase in inflammatory cytokines. More relevant here, several of the more common mycotoxins cause downregulation of mucin production by decreasing MUC2 and MUC5AC.[ref]
Vitamin D deficiency:
Low levels of vitamin D are a risk factor for inflammatory bowel diseases. Animal studies clearly show that vitamin D is involved in strengthening tight junctions in the intestinal epithelium. In an animal model of IBD, researchers found that the vitamin D receptor (VDR) is essential for mucosal repair in the small intestines.[ref]
Physical stress:
A number of studies show that there is increased intestinal permeability and mucosal damage after physical exercise stress (e.g. marathon running, extreme biking challenges). Extreme physical stress from being burned or badly wounded can also cause mucosal damage, as can the stress of pregnancy and childbirth.[ref]
Chronic psychological stress:
Animal studies show that sustained psychological stress causes decreased intestinal barrier function through the downregulation of goblet cells. Decreasing goblet cells directly decreases intestinal mucus formation.[ref]
Microplastics and nanoplastics:
A study in animals showed that exposure to microscopic bits of polypropylene plastic (< 10 μm) affects the gut mucosal barrier. The study showed decreased mucosal secretion and damage to the tight junctions, which then caused inflammation. Microplastics and nanoplastics (even smaller bits) are ubiquitous in packaged foods and in municipal water supplies.[ref]
Related article: Microplastics Research Roundup
Genotype report: Mucin producing genes
Lifehacks for optimizing your gut mucosal barrier:
Your gut mucosal barrier function depends both on your diet and lifestyle as well as the more minor role of genetic variants. For this topic, I would look at genetic susceptibility as being additive to dietary intake of surfactants, physical stress, mental stress, and mycotoxins. In other words – the information in this Lifehacks section likely applies to everyone to some extent, but with added susceptibility, if you have MUC2 or MUC5AC variants.
First, we will take a look at removing the negatives — surfactants and emulsifiers that damage the mucosal barrier as well as supplements that may be a problem for some people. Then we will look at the positive side of how to increase the mucosal barrier.
Removing surfactants and emulsifiers from your diet:
I’m going to ‘name names’ here and call out the specific emulsifiers that have been shown in research studies to impact the gut mucosal barrier.
A 2021 study investigated the effects on the intestinal mucosa and microbiome of 20 different dietary emulsifiers. Carboxymethylcellulose and polysorbate 80 had been shown in multiple prior studies to thin the mucosal barrier, but this study went further and looked into other common processed food emulsifiers.
The results showed that different dietary emulsifiers affect the gut in different ways. For example, the study found that “CMC [carboxymethylcellulose] impacted microbiota composition in a non-reversible manner, while DATEM and lambda carrageenan impacted three parameters in a reversible manner. Propylene glycol alginate impacted metatranscriptome and microbiota composition in a non-reversible manner.”
It also found that “Locust bean gum, HPMC, guar gum, and kappa carrageenan impacted various parameters in a reversible manner, while xantham gum, sorbitan monostearate, glyceryl stearate, maltodextrin, and P80 [polysorbate 80] impacted various microbiota parameters, both compositionally and/or functionally, in a non-reversible manner”. Encouragingly, soy lecithin and mono- and diglycerides did not show strong negative effects on the gut.[ref]
Examples of emulsifiers in foods:
Here are a few quick examples so that you know what you’re looking for in the ingredients lists.
Dairy Queen ice cream ingredients: Vanilla Reduced Fat Ice Cream: Milkfat And Nonfat Milk, Sugar, Corn Syrup, Whey, Mono And Diglycerides, Artificial Flavor, Guar Gum, Polysorbate 80, Carrageenan, Vitamin A Palmitate [ref]
Vlasic dill pickles ingredients: Cucumbers, Water, Distilled Vinegar Less Than 2% Of: Salt, Calcium Chloride, Polysorbate 80, Natural Flavor, Turmeric Extract (Color)
Soft Taco Flour Tortillas: Enriched bleached wheat flour, water, vegetable shortening, salt, sugar, leavening, distilled monoglycerides, enzymes, wheat starch, calcium carbonate, antioxidants, cellulose gum, guar gum, dough conditioners, and calcium propionate and sorbic acid[ref]
Hidden Valley ranch dressing: Ingredient List: Vegetable Oil (Soybean and/or Canola), Water, Buttermilk, Sugar, Salt, Egg Yolk, Less than 1% of: Spices, Garlic (Dried), Onion (Dried), Vinegar, Phosphoric Acid, Xanthan Gum, Modified Food Starch, Monosodium Glutamate, Natural Flavors, Disodium Phosphate, Sorbic Acid and Calcium Disodium EDTA Added to Preserve Freshness, Disodium Inosinate & Guanylate.
Krogers cottage cheese: Cultured skim milk, cultured cream, whey, salt, potassium chloride, maltodextrin, citric acid, carrageenan, guar gum, locust bean gum, cultured dextrose, sorbic acid (to maintain freshness), natural flavors.
In addition to thinning the intestinal mucosa, polysorbate 80 as a dietary emulsifier has been shown to decrease the production of MUC2.[ref][ref]
From Scratch: Yeast vs. Sourdough Bread
The obvious solution for avoiding emulsifiers and surfactant additives is to bake and cook at home from scratch.
However, if you’re baking at home, be sure to check the ingredients in your yeast (this one surprised me!). Sorbitan monostearate is included in some (all?) active dry yeast. Sorbitan monostearate is mentioned in the study above as impacting the gut microbiome and increasing pro-inflammatory signaling in the gut.
Sourdough instead of active dry yeast? A study looking at baking bread with yeast vs. sourdough bread found that sourdough was superior for the effects on the gut microbiome, including enhancing the synthesis of short-chain fatty acids.[ref] If you want to know more about the impact on the gut microbiome, the benefits of sourdough, and an in-depth look at different sourdough techniques, check out The Sourdough School. They have a unique perspective on learning to bake as a foundation part of lifestyle medicine.
Alcohol and the gut mucosa:
Just like rubbing alcohol is great for cleaning sticky stuff off your kitchen counter, alcohol is great at thinning out and breaking down your intestinal mucosa. One reason that excess alcohol consumption damages the liver is due to bacterial translocation from the gut due to the decreased mucosal barrier.[ref]
Supplements that may contain surfactants:
Prescription medications often deliberately include surfactants to thin the gut mucosa for better absorption of the medication. If you’re on a prescription medicine that includes a surfactant, talk with your doctor before making any changes.
OTC medications, such as ibuprofen also may contain surfactants, such as polysorbate 80 (Tween 80), sorbitan, PEG, or sodium laurel sulfate. Look at the Inactive Ingredients section on your OTC medications. You can also search on Daily Med for the brand name for FDA-approved products in the US. The listing lets you easily see the inactive ingredients (since it can be hard to read on some labels).
Again, medications and some supplements are deliberately manufactured to cause mucosal barrier thinning so that more of the product will be absorbed into the body. Without the mucosal thinning, you may not get the effect of the medication/supplement that you want. Thus, there are tradeoffs and you will want to consider how often you take the drug as well as whether you want to take it at the same time as food (and digestive enzyme production).
What about bile salts? Or bile supplements?
Bile salts are released from the gallbladder to help break down fats. Some bile salts (chenodeoxycholate and hyodeoxycholate) act as surfactants, and the natural release of these bile salts from the gallbladder will trigger the secretion of more mucus to counteract the mucosa thinning effect. This is how the intestines adapt to eating foods and having bile released for every meal. However, ursodeoxycholate (UDCA), cholate, and tauroursodeoxycholic acid (TUDCA) do not act as surfactants.[ref][ref]
I’ve included this because TUDCA is a common supplement for people with digestive or gallbladder issues, and it seems like it shouldn’t cause mucosal barrier thinning. I could not find any information on whether ox bile supplements, though, cause mucosal thinning.
What about Akkermansia muciniphila probiotics?
The gut microbiome is complex with a lot of different factors involved. Studies on Akkermansia muciniphila show that it is associated with a lower risk of obesity — and it is currently heavily promoted as a probiotic for weight loss. However, it is a bacteria that breaks down mucin and degrades the intestinal mucosa. An excess of Akkermansia muciniphila is associated with IBD, but the details of which strain of A. muciniphila may matter. Specifically, studies on the specific strain used as a probiotic show decreased inflammation.[ref][ref] Balance matters here, and it may be that some people should be cautious with A. muciniphila. If you want to know more, I highly recommend this review article on A. muciniphila, which dives into the details of when it is beneficial and when it could be problematic.
Dietary changes to improve mucosal thickness:
In addition to the big dietary change of removing foods containing added surfactants and emulsifiers, the following dietary interactions play a role in mucosal barrier function.
Fiber:
Animal studies show that dietary fiber increases MUC2 production and increases the mucosal barrier. Dietary fiber is used by commensal bacteria as a food source, and feeding the ‘good bugs’ helps to promote overall gut health.[ref] This is one of those dietary changes, though, that I would caution is complex and likely very individual as to exactly how much dietary fiber is helpful in the gut.
Mineral consumption:
The CLCA1 gene encodes an ion channel that is involved in mucin secretion from goblet cells. A study on mineral waters that contained various amounts of calcium, sodium, magnesium, and bicarbonate, showed that the increased mineral content from the water helped to protect the intestines from inflammation.[ref] This may be something to consider if you are lacking in minerals, including calcium and chloride.
Supplements for improving mucosal barrier function:
l-Glutamine:
Often recommended for gut problems, l-glutamine has been shown in several clinical trials to improve intestinal barrier function by increasing the health of cells lining the intestinal wall.[ref][ref] Glutamine is readily available as a powdered supplement. It doesn’t have much taste and is easily added to coffee or a drink.[ref]
Melatonin:
Melatonin acts as a potent intracellular antioxidant. In a mouse model of stress, the decrease in intestinal mucosal barrier thickness was accompanied by a decrease in melatonin levels. Supplemental melatonin was able to reverse the negative effects of stress on mucosal barrier thickness.[ref]
Vitamin D:
A deficiency of vitamin D is associated with a decreased mucosal barrier in animal studies.[ref] Thus, if you are vitamin D deficient on a blood test, increasing your vitamin D through sun exposure or supplements may help your intestinal barrier.
Licorice extract:
Flavonoids in licorice increase the regeneration of mucin-producing cells and also increase the mucosal barrier.[ref] Licorice extract is available online or in health stores and can easily be added to hot herbal tea.
Bee Propolis:
Several animal studies show that bee propolis increases the intestinal mucosal barrier. [ref][ref][ref]
Vitamin A:
Vitamin A is important in intestinal barrier function. For someone who is vitamin A deficient, increasing vitamin A should promote the mucosal barrier.[ref]
Check your genetic variants related to beta-carotene conversion in order to understand which type of vitamin A (beta-carotene or activ retinol forms) is more likely to increase your vitamin A levels:
| Gene | RS ID | Effect Allele | Your Genotype | Notes About Effect Allele |
|---|---|---|---|---|
| BCO1 | rs7501331 | T | -- | Decreased beta-carotene conversion to active form of vitamin A |
| BCO1 | rs12934922 | T | -- | Decreased beta-carotene conversion to active form of vitamin A |
| BCO1 | rs11645428 | G | -- | GG only: lower beta-carotene conversion to active form of vitamin A |
| BCO1 | rs6420424 | A | -- | Decreased beta-carotene conversion to active form of vitamin A |
| BCO1 | rs6564851 | G | -- | Decreased beta-carotene conversion to active form of vitamin A |
| BCO1 | rs119478057 | T | -- | rare mutation linked to hypercarotonemia and low vitamin A |
Zinc:
Zinc carnosine has been shown to stabilize the gut mucosal barrier.[ref] If you are deficient in zinc, adding in more zinc-rich foods or supplementing with a little zinc may help improve your gut mucosa. Below are your genes from the zinc article:
| Gene | RS ID | Effect Allele | Your Genotype | Notes About Effect Allele |
|---|---|---|---|---|
| IL-6 | rs1800795 | C | -- | C/C: additional zinc may not be needed in aging; G allele (common) may benefit from more zinc |
| SLC30A8 | rs13266634 | T | -- | Zinc may decrease blood glucose (if high) |
| SLC30A8 | rs11558471 | A | -- | Zinc may decrease blood glucose (if high) |
| SLC30A2 | rs587776926 | C | -- | Zinc transporter deficiency |
| SLC30A2 | rs185398527 | T | -- | Zinc transporter deficiency |
| SLC30A2 | rs117153535 | A | -- | Zinc transporter deficiency |
| SLC39A2 | rs2234632 | T | -- | Zinc reduces inflammation |
| SLC39A13 | rs121434363 | A | -- | Mutation linked to Ehlers-Danlos, zinc dependent |
| CA1 | rs1532423 | A | -- | AA: higher serum zinc |
Lactobacillus probiotics:
A new study shows that Lactobacillus probiotics, specifically L. plantarum can help to improve the gut mucosal barrier. One way that they do this is through binding to and removing microplastics.[ref]
Recap of your mucin-related genes:
| Gene | RS ID | Effect Allele | Your Genotype | Notes About Effect Allele |
|---|---|---|---|---|
| MUC2 | rs11825977 | A | -- | decreased relative risk of inflammatory bowel diseases; decreased risk of Parkinson's; likely higher MUC2 expression (interpretation) |
| MUC2 | rs2856111 | C | -- | slightly increased relative risk of IBD; likely lower MUC2 expression (interpretation) |
| MUC2 | rs7396030 | G | -- | G/G: increased MUC2, increased risk of gallstones |
| MUC5AC | rs868903 | T | -- | increased relative risk of stomach cancer |
| MUC5AC | rs16866419 | C | -- | decreased MUC5AC production (GWAS study) |
| MUC5AC | rs75401036 | A | -- | decreased MUC5AC production (GWAS study) |
| MUC5AC | rs75401036 | A | -- | decreased MUC5AC production (GWAS study) |
| MUC5AC | rs2688513 | G | -- | higher mortality rate in colorectal cancer |
| CLCA1 | rs2734705 | G | -- | G/G: likely more mucin secretion; increased risk of intestinal ileus (lack of motility) in infants with cystic fibrosis |
Related Articles and Topics:
Longevity Lifehacks articles on Intestinal mucosal barrier and breakdown in aging and Autodigestion?